Obgyn History Template
Obgyn History Template - Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. What birth control method(s) do you currently use? Obstetrical history including abortions & ectopic (tubal) pregnancies. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we.
What birth control method(s) do you currently use? Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Obstetrical history including abortions & ectopic (tubal) pregnancies. Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we.
Obstetrical history including abortions & ectopic (tubal) pregnancies. Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. What birth control method(s) do you currently use?
History Taking Template
Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Obstetrical history including abortions & ectopic (tubal) pregnancies. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number.

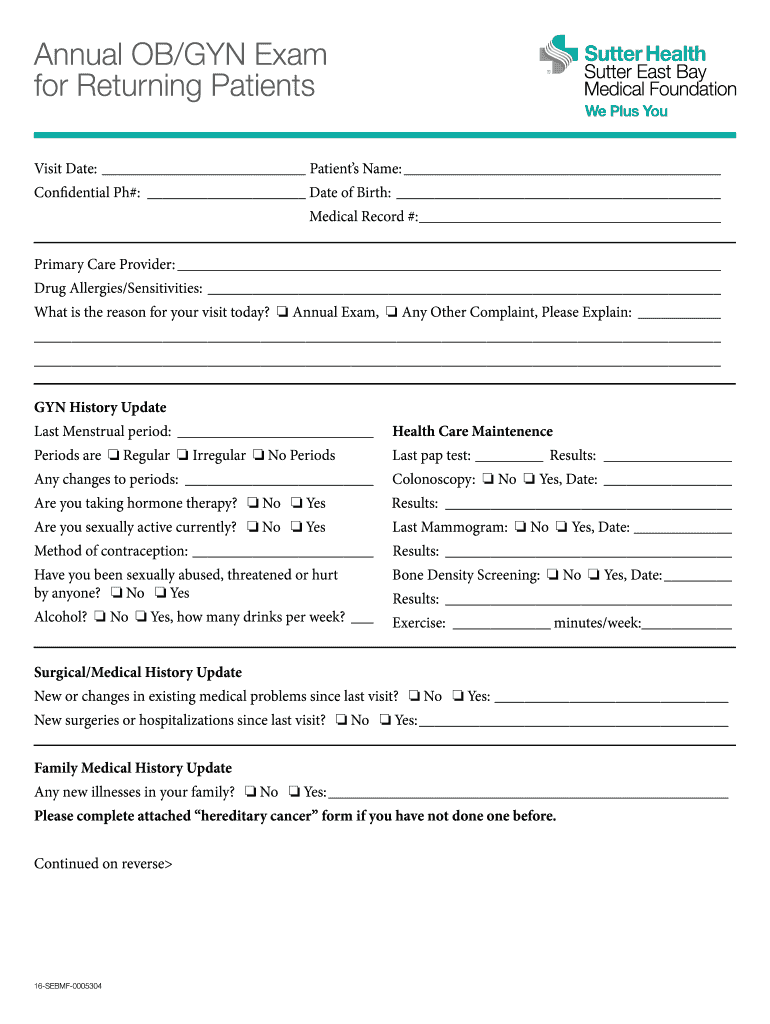
OBGYN West Health History Form Fill and Sign Printable Template
Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology. Obstetrical history including abortions & ectopic (tubal) pregnancies. What birth control method(s) do you currently use? Obstetrics and gynecology medical history questionnaire.
Ob History And Physical Template Card Template
Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Obstetrical history including abortions & ectopic (tubal) pregnancies. Medical history questionnaire department of obstetrics & gynecology division of.

OBGYN Patient History Form Template OnTask
Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. Obstetrical history including abortions & ectopic (tubal) pregnancies. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Medical history questionnaire department of obstetrics & gynecology division of.
Ob Gyn History Template
Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. Obstetrical history including abortions & ectopic.
Obgyn History Template
Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. Obstetrical history including abortions & ectopic (tubal) pregnancies. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form.

Obgyn History Template
Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. What birth control method(s) do you currently use? Obstetrical history including abortions & ectopic (tubal) pregnancies. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Medical history.
Obgyn History Template
Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. What birth control method(s) do you currently use? Obstetrical history including abortions & ectopic (tubal) pregnancies. Medical history.

Obgyn History Template
Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. What birth control method(s) do you currently use? Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form.
Ob Gyn History Template
What birth control method(s) do you currently use? Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. Medical history questionnaire department of obstetrics & gynecology division of.
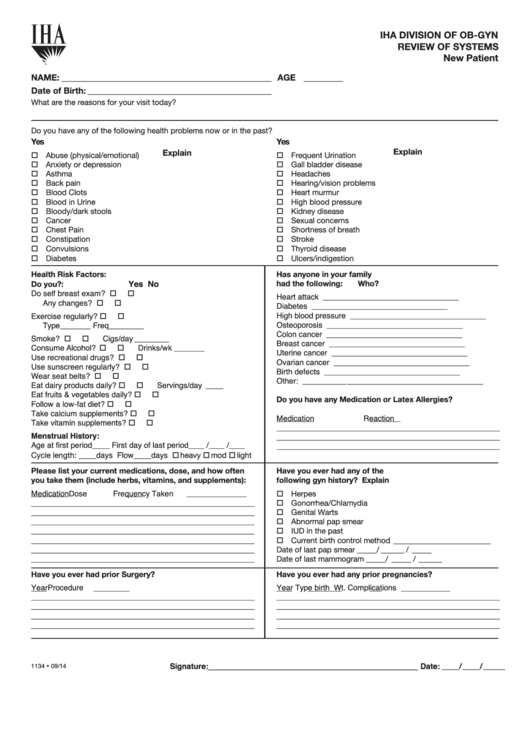
Medical History Questionnaire Department Of Obstetrics & Gynecology Division Of Reproductive Endocrinology.
Obstetrical history including abortions & ectopic (tubal) pregnancies. What birth control method(s) do you currently use? Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020.